 When my daughter was younger, I had this notion that parents who had adult children with developmental disabilities living in a group home or other setting had crossed some kind of finish line, as if their intensive effort of many long years had resulted in success. They were able to safely hand off the day-to-day support of their children to others who were unimpeded by aging bodies and exhausted minds. Perhaps for some parents, this is true. But I don’t think it is for most of the parents of children with severe developmental disabilities that I know. It definitely isn’t for me. I’m afraid that there may be no such thing as a finish line, or a time that making sure that Lauren’s intense and diverse needs are met, won’t be primarily up to me.
When people I haven’t seen for awhile inquire about my daughter, I say, “Lauren’s doing well! She’s living on her own now.” Of course, then I have to explain that “living on her own” means that someone is with Lauren 24/7 to support and care for her. I usually don’t include the other fact that “living on her own” requires my constant oversight and management of every facet of her life. Lauren may no longer live under the same roof as I, but she still depends on my constant presence in her life. Since Lauren has a severe intellectual disability, as well as severe physical disabilities, she depends on someone to know her well enough and care about her enough to make decisions, guide her choices, and protect her health and well being. That would be me. Eight years ago when I was making this adult living concept a reality for Lauren (her own rented home with 24/7 staffing), I mistakenly believed that this distance between us—her in one house, me in another—would also create space between the worries and anxiety that were a constant presence when she was home. It has not. I still worry about all of the same things, plus now I feel constantly in a no man’s land in the war between my need to support her in an independent adult life, and my need to have her within easy reach and under my watchful eye. Sometimes I think it would be less stressful to just bring her back home, eliminate our “separateness”. Then I would be able to monitor every moment of her life. I would be able to touch her, to look into her eyes, to ponder the subtle intonations of her vocalizations. But I cannot give in to that because it would be selfish. Lauren does not live in a home of her own because I do not want her living in mine. No, Lauren lives in a home of her own because she needs to build an adult life in which she can survive without me. This arrangement is the first step. It’s not perfect because I am still so heavily involved in her life, providing support I won’t be here forever to provide. But this is a good first step, because while I’m still involved in the days of her life, I am not involved in the minutes. Those minutes are under the watchful care and support of the wonderful Direct Support Professionals (DSPs) that Lauren has in her life. They know her well and provide consistent and diligent care, but no DSP will ever know her as well as I do. She may have five other people facilitating those moments in her days, but I have the final responsibility of figuring out if a question or concern is “something” or nothing. A vocalization could mean anything from I’m in pain to I don’t like that song. A pale face could mean I don’t feel well, I’m tired, or It’s too warm in here. A refusal to eat could mean I’m feeling nauseous, I don’t like that sandwich, or I want the television on. The possibilities of Lauren’s subtle cues are endless. When a DSP can’t figure out what’s going on with Lauren, it’s up to me to figure it out.....or to make an educated guess. Lauren’s care places a lot of responsibility on the shoulders of the DSPs, but I still hold most of the clues to the messages hidden in Lauren's wordless existence. And so, though even I am not always right, the final judgment on everything rests with me. Lauren recently had a little cough. It wasn’t getting better. But, it wasn’t getting worse either....until suddenly, on a Sunday of course....it started to sound different. I jumped in the car at eight o’clock at night, because in speaking to two different DSPs who had just changed shifts, I was getting two differing reports on Lauren’s condition. Lauren was definitely worse, but call-the-doctor-in-the-morning worse not a rush-to-the-ER worse. I ended up staying through the night to monitor her, to try to make her comfortable while the cough was interrupting her sleep. Lauren doesn’t get sick all that often. Her DSPs just don’t have as much experience as I do with helping her weather an illness. Lauren’s doctor—who sees her for maybe fifteen minutes a couple of times a year—does not know Lauren well enough to “read” her in anyway. And, whether the doctor is saying, “Take a deep breath” or “Open your mouth”, I have to explain that Lauren doesn’t understand her instructions and help her get the result she needs. Since the doctor is looking at an individual who is so atypical of the majority of her patients, it’s up to me to decipher for her what is typically atypical for Lauren and what is not. And, since Lauren cannot tell us what she is feeling, it’s up to me to guess and relate that to the doctor. She must then consider my input with her exam, made with the limited cooperation of Lauren, in order to come up with a diagnosis. It’s not the ideal scenario. The doctor prescribed an antibiotic for an upper respiratory infection and an antihistamine to control the mucous. The antihistamine allowed Lauren to have the first decent night’s sleep in awhile, but left her too groggy to eat the next day which she primarily slept through. The antihistamine had to be discontinued. I’m hoping the antibiotic kicks in soon, because she’s still not herself and I can’t stop worrying that I’m missing something until she is. So while we wait for this wonder of modern medicine to hopefully start working, I’m on the phone, talking and texting, with the DSPs, issuing instructions, and trying to walk the fine line between trusting those very able DSPs to care for Lauren and wanting to do it myself. Yesterday, when I stopped in and sat for an hour next to a clearly fatigued and pale Lauren, the DSP said to me, “You really have to stop staring at her.” And, she was right. I was unnecessarily focused on Lauren’s thin form as if some nuance of her breathing or the distinct shade of her pale cheek held some critical message I couldn’t miss. I need to give her the time she needs to rest and recuperate, but I can’t stop worrying that she’s actually not getting better......and I’m not seeing it. I talk about that hypervigilance in my recent post on PTSD in parents of children with developmental disabilities. There are no days that I do not wait for the phone to ring or wonder why the phone hasn’t rung. It’s just the reality of this arrangement. I am in charge of guiding Lauren’s experience of life, her ability to travel safely through her days. Normally, I physically visit her two or three times a week. There are often times when I feel that she doesn’t seem quite right, but I can’t figure out why. So I dwell on it for the rest of the day weighing possibilities, fearing possibilities....until I can check on her again. Hopefully, I find out that she was fine after I left. What she needed was for me to leave. Sometime she makes that quite clear by pushing me away when I lean down to plant a smooch on her cheek. I’m interrupting her day. Thankfully, there are other days when all is well, and I sit on her couch with her as she leans into me resting her head against mine. It’s a “mom moment” I live for and the sun shines the rest of the day, regardless of the actual weather. I can’t believe it’s been almost eight years that Lauren has been on her own. I expected it would get easier, more mundane at some point. It has not. Lauren really loves this life on her own. She doesn’t even want to come home to visit anymore. It’s as if my home is a “been there, done that” place in her life that she doesn’t need to revisit. It kind of hurts. But I’m also really proud of her. This bit of independence shows a maturity of which I didn’t think she was capable. But, there is always something tearing at the fragile web of stability that is Lauren’s life. If it is not a problem directly with Lauren, it’s a problem with staffing, funding, new rules, or old equipment. Lauren’s well being is not just dependent on her physical care, I am also responsible for making all of the ancillary details of Lauren living on her own coordinate to support her life – finances, staffing, housing, transportation, etc. So when I share my news with people and they react with “Oh, that’s great!” I agree, at least in theory. I don’t think they can understand the investment of my time and knowledge that it takes for Lauren to successfully live on her own. I don’t think they will grasp how very mixed my emotions are about this situation. As I wrote in Special Needs, “....I feel selfish that I am not with her every moment to ease her way through this challenged life that I have given her. Is it my responsibility to prepare her to live without me? Or, is it my responsibility to dedicate my every waking, and sleeping, moment to personally assuring her comfort and safety? Somehow, it’s both and that’s impossible. I know that. And still, I feel guilty.” So I have loosened my grasp on the minutes of Lauren’s life, but as of yet, there is no one who can be “me” when I have ceased to be, and there is no entity within the system of supports prepared or designated to become me when needed. This finish line that I thought was something that parents reached is in reality something their children reach—the ability to live independently of their parents. It’s a finish line that Lauren depends on me to help her reach, and that is definitely an added worry, because I don’t see it anywhere on our horizon.
0 Comments
Isn’t it Sad....That We Need to Compel Others to Care about Adults with Developmental Disabilities?3/20/2019  In Special Needs, I wrote about some of the comments that my daughter and I frequently get from community members who encounter us during the course of their day. In between the “I’m so sorry for you.” and the fervent “God bless you” responses, there are the sad but furtive glances steered our way. People mean well. They think they understand, but really, they don't. They do not realize that although Lauren’s life is severely challenged and our life together is far from easy, the saddest part of our journey is actually the challenges and roadblocks added by the world around us to the challenges with which Lauren was born: the hurdles of finding, keeping, and managing necessary supports and services, the difficulties in finding providers—medical and otherwise—who can and will address needs, and the indifference, ignorance, and community barriers we all too often encounter.
Because my life, by necessity, has become so embroiled in everything “disability”, I sometimes forget that the majority of people have no idea what life is like within the developmental disability community. They are truly surprised that you can’t just ask for what you need in order to obtain it. They also believe that when our children want or need to live somewhere other than the family home, options are easily and readily available. Sometimes I don’t think they believe me when I explain that our communities are not prepared to care for individuals with developmental disabilities. They don’t realize that homes, activities, jobs, medical care, and people to provide the care we parents cannot continue to provide for a lifetime, are significantly lacking. Disability-rights activist Karin Hitselberger recently wrote, "Disability means having to figure out every day how to function in a world that consistently forgets you." Strangers, and sometimes family members, often approach me as if Lauren is a tragedy that has occurred in my life. They speak of reverence of our journey and express that they could never endure the parenting journey I am on. I can understand their fear. I can understand that their inexperience renders them unknowing, not uncaring. What I don’t understand are the people who should know better, yet do not feel compelled to care. I find that incredibly sad. It is sad that the New Jersey Assembly has recently felt it necessary to approve a proposal for a bill of rights for families of individuals with developmental disabilities. The bill seems to be directed at how state agencies, tasked with providing services and supports, treat family members of individuals. I find it very distressing that this issue was deemed such a significant need by the legislature that they took this step to assure that state agencies operate with civility, truth, and compassion toward vulnerable individuals and their families. As Assemblywoman Downey said, “Some of these are things that should be common sense.” A few of the rights outlined in the bill are: The right to be treated with consideration and respect The right to receive return phone calls within a reasonable time frame The right to be given understandable and honest information The right to be free from retaliation if a complaint is made Isn’t it sad that these things had to be spelled out as requirements? A press release stated that the bill of rights will be distributed by the Division of Developmental Disabilities to case managers and “...posted in a conspicuous place in each office of the Divisions of Developmental Disabilities and Disability Services in the Department of Human Services, in each State developmental center, and in adult group homes overseen by the DDD.” But, there are no details about who will judge whether these rights are respected or not. There are no details about what the repercussions will be if they aren’t? Will this bill of rights be “posted” on walls where it will become faded and forgotten—like old wallpaper no one notices anymore? Something else that should be a right—dental care—has long been a struggle to find for individuals with developmental disabilities. Most dentists will not see these individuals. Recently, I read the headline, “Dentists no Longer Permitted to Turn Away Patients with Disabilities” and reacted with Wow, that’s great!. And then I stopped myself. How could this have been permitted in the first place? Why has it taken this long for the American Dental Association to compel dentists to care about the dental health of individuals with developmental disabilities? Within the article it noted that dentists were concerned about the amount of time it would take to treat people with intellectual and developmental disabilities. Jane Koppelman, a senior manager of the dental access campaign for the Pew Charitable Trusts stated, “Sometimes it’s difficult to have a patient in the chair if they are very, very anxious about being treated, if they have difficulty sitting still or if they feel a lot of fear, and sometimes those circumstances are more prevalent in people with varying disabilities.” This seems to imply that it is the dentist that deserves our sympathies....not the frightened patient. I think the individual in pain or discomfort because no one will care for their teeth is the person who deserves our sympathies. How has the dentist been prepared to treat all members of his community not just the easy ones? How have dental schools prepared their students to deal with physical, cognitive, sensory, and behavioral issues? A mother looking for dental care for her child with autism asked in an online health forum if it was legal for one dentist after another to deny her son care. A dentist responded, “...the dental profession and its educational system as a whole have been grossly negligent in producing doctors who are able to treat such patients. ...the dental profession....is just not geared toward accessibility for disabled patients simply because the majority of dental professionals just don't think the effort it takes to treat them is worthwhile.” Wow. Isn’t that sad? I experienced this refusal to treat with my daughter many years ago. Our family dentist wouldn’t see my tiny four-year-old because she had disabilities. Fortunately, I was able to find a wonderful dentist – an hour away – who treated her for many years. That dentist has now retired and next week I’ll find out if his successor will be as caring and accessible going forward. Moving forward into an uncertain future is scary on so many levels for most parents of children with developmental disabilities. And, in this age of instant communication and social media, our fears are informed everyday by not only our current problems and our memories of past hurdles and injustices, but by our constant connection to the experiences of others. Today’s advanced ability to connect and share information has become a vital resource for parents, but it also provides a seemingly endless inventory of all that can and does go wrong in our children’s lives—abuse, neglect, inadequacy of supports, and the decline of once stable lives. For every one positive story there are ten that rip your heart out. I know that although I am exhausted by this never-ending battle, I have no choice but to continue to compel others to care whenever I can. But, there shouldn’t have to be advocacy to gain rights and respect for people who should never have been without them in the first place. I look at my Lauren who has lived with grace and simple acceptance of overwhelming challenges for all of her thirty-three years and I wonder, Who can deny that she is worthy of their admiration and best efforts to assure that her life is not further wounded by their actions.....or inactions? But the voices of advocates are all too often not much more than a whisper amongst the clamor of the many issues competing for the attention of people who hold our fate in their hands. Our president has just submitted a budget that includes deep cuts to Medicare and Medicaid – the primary funding source for disability services and supports. Over a decade, President Trump’s plan would reduce Medicare by over $800 billion and cut Medicaid spending by $200 billion. The plan also calls for cutting programs such as independent living programs, respite care, and state councils on developmental disabilities. It would seriously cut funding for Special Olympics and do away with a $51 million initiative to address the needs of those with developmental disabilities and autism. Opponents of his plan say these cuts are being used to make up for the revenue shortfalls created by corporate and individual tax cuts passed in 2017. Individuals with developmental disabilities and their families can only hope that someone in Washington will be compelled to care that they do not become collateral damage. And like all too many other things.......Isn’t that sad?  Every single time my cell phone rings, my heart starts to thud in my chest. It feels like it’s trying to escape the muscle and bone that contain it. Slightly light-headed, I can’t grab the phone fast enough to see the caller ID, often fumbling with the wrong side up, upside down phone in my haste to read the screen. A mantra runs through my brain, Let it not be them, let it not be them, “them” being whoever is caring for my daughter at that moment. My ding-dong text alert results in the same response. Crazy thing is, this happens even if I’m with Lauren—my body’s learned response akin to Pavlov’s dog. It’s the result of too many years of a ringing phone being a call to arms, or rather a call to run. And if not necessitating a mad dash out the door, at a minimum, the ring signals some problem or issue affecting Lauren’s well being.
Lauren’s early years were such an uphill battle, so strewn with things for me to panic over, that panic has become my default response to even the potential of a problem. It’s probably some primitive, fight or flight response, helping me prepare for even the possibility that heightened preparedness is needed. And, it’s exhausting. In a recent post, when referring to parents raising children with severe developmental disabilities, I used the phrase, ”the post-traumatic stress of raising their child to the present day...”. Do parents actually develop post-traumatic stress disorder (PTSD)? Can parents on this difficult journey suffer from something we more frequently associate with veterans of combat and military operations? Researchers are beginning to study the effects that raising a child with a life-threatening or serious and chronic conditions can have on parents. Studies have measured the cortisol levels of parents of children with disabilities and found them comparable to individuals who have been diagnosed with PTSD. Cortisol is a hormone that regulates many of the body’s processes including metabolism and immunity. These increased levels of cortisol put individuals at risk for compromised mental and physical health. It may result in fatigue, decreased immunity, mood disorders, poor sleep, headaches, gastrointestinal problems, and increased vulnerability to stroke, heart disease, and hypertension. The American Psychiatric Association defines PTSD as a psychiatric disorder that can occur in people who have experienced or witnessed a traumatic event, something that is generally outside the range of usual human experience. Most parents of children with developmental disabilities have had ample evidence over the years that their parenting experience is far from the norm. The clinical criteria for the diagnosis of PTSD is a lengthy list that explores the nature of the exposure, the presence of symptoms such as flashbacks, reactions to related events, and prolonged distress. It also looks at negative alterations to cognition and mood, symptoms such as hypervigilance, irritability, sleeplessness, and the duration of all of these symptoms. Everyone reacts differently to the “outside the range of usual human experience” experience of raising a child with developmental disabilities. And, no two experiences are exactly the same. Our children, their unique challenges, our families, our culture, our communities, its resources, and our own personal resources and challenges all contribute to our individual experience of raising a child with special needs. The development of PTSD in a parent depends on all of those interrelating factors. Reports and studies specifically about the occurrence and prevalence of PTSD in parent of children with disabilities are few, but growing. Researchers note that a single traumatic event or the ongoing condition of a child can cause PTSD. Data from sixteen pooled studies show the prevalence of PTSD in parents of children with disabilities at 23%. Another study shows the prevalence at 30% with another 30-40% experiencing symptoms significant enough to impair function. Because these studies include parents of children with all disabilities and medical conditions—not just developmental disabilities—the true prevalence specifically in that subgroup is unknown. Parents tend to develop an exclusive focus on their child’s life management and well-being—totally engaged in their child’s challenged experience of life. An interesting survey by anthropologist David Marlowe has shown that witnessing harm to, or the distress of, others is actually more traumatic to an individual than experiencing danger or trauma themselves. Parents do not make their own well being a priority, nor is it the priority of professionals caring for the child. In order to facilitate connections and solidarity among parents having similar experiences, parents, especially in the early days, are sometimes referred to support groups where they can share their experiences with each other. I had my own experience with a well-meaning group that was part of Lauren’s Early Intervention Program. I wrote about it in Special Needs, “There are a lot of tears and monologues of woe in this stuffy room, and the hands on the clock above the door, which is our only escape, move all too slowly. It is consistently painful to listen to the heartbreak of these mothers, of their dashed dreams and unrealistic hopes.” It’s been found that the sharing of similar experiences may actually add to a parent’s trauma by adding other’s experiences to their own, reinforcing trauma rather than providing positive reinforcement. When it comes to caring for and protecting your child— from an evolutionary perspective—it’s good to sleep lightly, wake quickly, react to strange noises and generally be vigilant. Anger keeps you ready to react; flashbacks are a reminder of potential threats. But this is usually a short term response, not a life-long need. It’s been said that in this type of survival mode, you don’t thrive. You simply endure. Fellow mom, advocate, and blogger, Hillary Savoie, has said, “If your child’s health status is unchanged for the duration of their life or your own, how do you reorient yourself to regular life while remaining in anticipation of the repeat of a traumatic event: The thing that is harming you is also helping you to protect your child.” I can’t help but believe that a contributing factor in parents developing PTSD is the fact that raising a child with developmental disabilities can be an intensely isolating experience—the child’s needs and challenges creating barriers to social connection and participation. In Sebastian Junger’s Tribes, a book on PTSD, he notes that “In humans, lack of social support has been found to be twice as reliable at predicting PTSD as the severity of the trauma itself.” He also notes that, “....one way to evaluate the health of a society might be to look at how quickly its soldiers recover, psychologically, from the experience of combat.” Perhaps we should look at the increasing evidence of the occurrence of PTSD in parents of children with developmental disability the same way. Of course, most parents are not experiencing traumatic events every day. There are family dinners, things to celebrate, and blissfully boring days. But, Junger further explains that the interweaving of trauma with positive experiences makes it difficult to separate the two. When this goes on long term it creates a more complex scenario than a traumatic event that is limited or isolated. And raising a child with developmental disabilities into adulthood is all too often a long-term series of traumatic events. I think if a diagnosis of PTSD becomes more prevalent in the lives of parents of children with developmental disabilities, they will have to adjust the name of the disorder. There is no “post” to the stress, trials, and fears of continuing to support our children through adulthood. Coping mechanisms for overcoming the effects of trauma will need to be adjusted for those who must continue to endure in a role where sustained threats and disturbing events never end. I’ve tried many coping mechanisms over the years, but the results are temporary, superficial, insufficient. My morning meditation is frequently interrupted by a text message from a DSP. I’ve even tried changing the ringtone on my phone to something bright and breezy, an audible reminder of the positive potential as well as the negative. It didn’t help. It brings to mind the phrase--putting lipstick on a pig.....I still knew what could be behind that ring. It is difficult to remember when anxiety became my default emotion, when constant vigilance became more a norm rather than a situational necessity. Having Lauren changed my life in a far greater way than just adding “Mom” to the roles I planned to have. I became “mother of a child with severe developmental disabilities” and it was far more than a new role. That reality colored every decision, event, and possibility in my life. It had the conflicting effect of both expanding my concept of who I was and who I thought I could be, and limiting the content of my days and opportunities in my future. But most of all, it changed my reaction to and perception of the world and my understanding of the dangers that lurked within it.....for my child, yes, but also for me, lest something render me incapable of caring for her. And perhaps most of all, it has resulted in unending vigilance and a disturbingly informed fear of what could easily happen next. Is that PTSD? I don't know. I do know that whatever you may call it, it will be with me until my thudding heart no longer continues to beat. 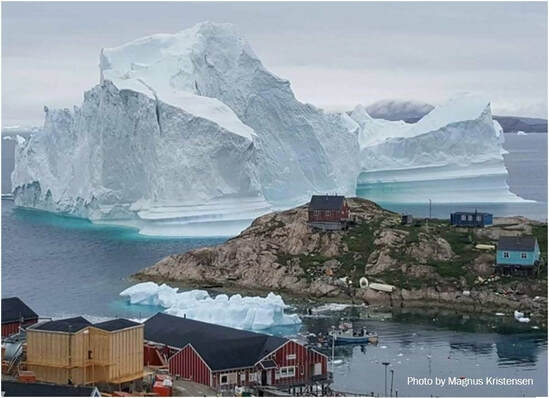 As I read a recent article by New Yorker staff writer, Carolyn Kormann, I couldn’t help myself from seeing a parallel between the threat the giant iceberg in her story represented, and the threat that the instabilities of the disability service system represents to families.
In Climate Change and the Giant Iceberg Off Greenland’s Shore Ms. Korman writes, “For a week, an iceberg as colossal as it is fragile held everyone in suspense. It arrived like a gargantuan beast that you hope won’t notice you, at the fishing village of Innaarsuit, Greenland, about five hundred miles north of the Arctic Circle. The iceberg posed a mortal threat to the village population of about a hundred and seventy people.... If a big enough part of it sloughed off, in a process known as “calving,” it would cause a tsunami, immediately destroying the little settlement on whose shore it rested.” Like that iceberg, the current resources for supports for adults with developmental disabilities are not actually a cohesive whole. That iceberg may look like a solid block of ice, but like these resources, it is actually full of cracks and fissures always in jeopardy of breaking into the disparate pieces that comprise it. Yet it is a wondrous presence for those who live humbly in its shadow..... until a piece breaks away. The loss of any piece that completes the puzzle of living as an adult with developmental disabilities can erode the stability and quality of an individual’s life. It can become a “calving” in an individual’s personal iceberg. Under the new Medicaid-based system of services we’ve just rolled out in New Jersey, a viable adult life requires piecing together supports and resources from multiple sources. That is mostly because Medicaid-based funding cannot cover expenses related to housing, utilities, or food. The majority of adults with developmental disabilities are going to need some type of residential option beyond the family home at some point in their life.....for the rest of their life. Any model that requires a piecemeal answer to the obvious need for adult residential options is problematic for individuals, who for the most part, will not financially or intellectually be able to create an independent life for themselves. The necessity of cobbling together resources and supports to meet the comprehensive needs of adults with developmental disabilities means that there are inevitable inadequacies and vulnerabilities in creating long-term, stable adult living solutions. There are pros and cons to this new Medicaid-based system. Aligning with Medicaid rules allows access to Medicaid matching funds bringing much needed federal revenue into the state developmental disability service system. However, aligning services and supports with Medicaid’s medical-model of billing and coding has created issues. It has eliminated the flexibility providers used to have in budgeting with known lump-sum funding. And, the rates assigned to services, which were determined by a lengthy and intricate process, were eventually funded below the recommended rates. For individuals who are self-directing, the fact that in this system funding is applied to individuals, rather than to programs, increases flexibility by putting the choice of how their funds are utilized (within strict parameters) in their own hands. But, completing the adult living puzzle for someone like my daughter means utilizing eight different resources—with different rules and access points—in order for all of her needs to be met. This piecemeal system of care is a frightening scenario when trying to establish acceptable long-term care options for adult children. It doesn’t matter if that option is under a provider’s wing or a self-directed option. We see provider’s struggling to make ends meet under this new system. How can that not affect quality of care if resources are insufficient? For families that have set up creative adult living options using multiple resources, each piece of that complicated puzzle is subject to change and is shifting constantly. Each year since Lauren moved into her own home there have been changes to the amount of funding, or rules governing the funding, of almost every single one of her funding resources. Keeping her life intact requires a delicate dance of sorts, moving and swaying to seemingly inharmonious notes, trying to maintain the balance and flow and budget of a stable life. I understand the trepidation of watching a hulking iceberg float wondrously yet menacingly nearby. As I wrote in Special Needs, “...the life my daughter is living is growing increasingly precarious. The systems that she depends on are constantly changing, and there is no guarantee that the supports she has today will continue to be there for her tomorrow.” Families who count among them a loved one with developmental disabilities are caught up in the same worries as all families. We’re inundated with non-stop news of political, financial, and social issues affecting our world. We just have the worries about the present and future of particularly vulnerable children on top of all that. All of these issues have the potential to trickle down to affect the resources we have no choice but to depend on to support the beyond-our-means, lifelong needs of adults with developmental disabilities. All of these issues could result in detrimental changes in our children’s lives, our children who have diminished ability to weather serious changes, especially when we can no longer help them. Change is not always bad. And yes, we need to serve the developmentally disabled population more effectively and efficiently. But as I’ve watched non-stop change in this system for the last thirty years, it seems as if our children and our families often seem to be used as nonconsenting test subjects for experiments in formulating viable service systems. Service systems are tasked with serving individuals adequately and equitably. That’s a lot to ask of a system serving this incredibly diverse population .....maybe too much. New systems seem to lack the adaptability of the former ones, the strict parameters and guidelines curtailing the option of using common sense to meet uncommon need or of preventing the unraveling of a stable life simply to suit newly instated rules. And it seems that each time change descends upon us, it is not something to endure and recover from. No, it is simply a temporary alteration not a long-term solution. We here in NJ, like many other states, have just spent years converting to a Medicaid-based “fee-for-service” (FFS) system. This was a drastic change from the former system and it was a difficult transition. The overall impact of the change is still to be determined. Now, we learn that a senior advisor to Health and Human Services Secretary Alex Azar recently stated that one of the prime goals of his position is to “blow up fee-for-service”, that is, to get rid of the Medicaid FFS model. This means that more change is definitely coming........again. Feedback on the FFS systems across the country is in. A 2018 survey by the Kaiser Family Foundation in all fifty states noted that achieving value, quality and outcomes, “... means moving away from FFS (Fee-for-Service) payments.” A recent report by ANCOR (American Network of Community Options and Resources), indicates that a FFS system does not work and does not improve quality or value in critical systems of services and supports. The report states an imperative that new systems must do something that current ones are not “...promote continuity and stability for individuals, families, and providers.” Wouldn’t that be amazing? What is the alternative to FFS? The ANCOR report points out that ten “alternative payment models” utilized in eight states across the country are not resulting in an improvement on FFS. These alternative models, in various stages of implementation, are insufficiently tested, measure outcomes inconsistently, and few are achieving savings. In addition, they share the similar issues of FFS - inadequate payment rates, a lack of desperately needed investment in the direct support workforce, and a lack of utilization of stakeholder input. No matter how diligent, creative, or intrepid we are as parents, it just never seems to be enough to ensure the security of our children’s futures. A new system, a new rule, or a funding change can arrive, and destroy or threaten, the hard earned stability or quality of our child’s life. Like the climate change that spawned this behemoth of an iceberg in Greenland, families are subject to something over which we have little personal control. My child is dependent on publicly-funded systems today and for all of her tomorrows. The fact that those supports exist is something for which I am incredibly grateful. What on earth would I do without these resources? But that dependency on something so ephemeral in its constancy is incredibly worrying. What if someday Lauren’s simple but comfortable life unravels because someone, who has never even seen the long-lashed brown eyes of a woman in a small town in New Jersey, changes a program or cuts critical funding? What if I have succumbed to the inevitabilities of aging and infirmities, and I cannot protect her? The weight of that hangs over my days like a storm cloud threatening a sunny day. I know there are many people diligently working to formulate systems and supports that will work for people right now. But that is their job for today. We’ve seen administrations on all levels come and go, leaving their successes and failures behind with our children and families. What is missing is a commitment to a tenet attributed to the Hippocratic school of thought, “...help or do not harm.” A demonstrated commitment to that would provide tremendous relief for families worrying about the long-term well being of their children with developmental disabilities. But, we are not there yet. So, I cannot help but worry about Lauren’s future dependent on resources with a long history of instability. And like the villagers of Inaarsuit I know my worries are not unfounded. Last summer, a neighboring village, Nuugaatsiaq, was inundated by a three-hundred foot wave. Now, the villagers of Inaarsuit have ample evidence, as we who endeavor to ensure safe and stable futures for our children do, that there are no guarantees when living in the shadow of an iceberg. |

Gail Frizzellis the author of Special Needs: A Daughter's Disability, A Mother's Mission. Gail is an accomplished advocate and writer in the field of developmental disabilities and Mom to Lauren, a young woman endeavoring to lead her best life despite severe challenges. Archives
September 2019
Categories |
 RSS Feed
RSS Feed